
Page 409 - The Vasculitides, Volume 1: General Considerations and Systemic Vasculitis
P. 409
Dermatologic Aspects of Systemic Vasculitis 383
to 8 years after diagnosis of systemic GPA, and others in whom the cutaneous eruptions
preceded systemic involvement by one to seven years [28].
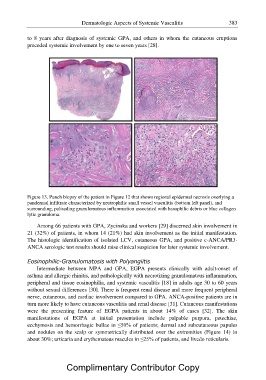
Figure 13. Punch biopsy of the patient in Figure 12 that shows regional epidermal necrosis overlying a
pandermal infiltrate characterized by neutrophilic small vessel vasculitis (bottom left panel), and
surrounding, palisading granulomatous inflammation associated with basophilic debris or blue collagen
lytic granuloma.
Among 66 patients with GPA, Zycinska and workers [29] discerned skin involvement in
21 (32%) of patients, in whom 14 (21%) had skin involvement as the initial manifestation.
The histologic identification of isolated LCV, cutaneous GPA, and positive c-ANCA/PR3-
ANCA serologic test results should raise clinical suspicion for later systemic involvement.
Eosinophilic-Granulomatosis with Polyangiitis
Intermediate between MPA and GPA, EGPA presents clinically with adult-onset of
asthma and allergic rhinitis, and pathologically with necrotizing granulomatous inflammation,
peripheral and tissue eosinophilia, and systemic vasculitis [18] in adults age 30 to 60 years
without sexual differences [30]. There is frequent renal disease and more frequent peripheral
nerve, cutaneous, and cardiac involvement compared to GPA. ANCA-positive patients are in
turn more likely to have cutaneous vasculitis and renal disease [31]. Cutaneous manifestations
were the presenting feature of EGPA patients in about 14% of cases [32]. The skin
manifestations of EGPA at initial presentation include palpable purpura, petechiae,
ecchymosis and hemorrhagic bullae in ?50% of patients; dermal and subcutaneous papules
and nodules on the scalp or symmetrically distributed over the extremities (Figure 14) in
about 30%; urticaria and erythematous macules in ?25% of patients, and livedo reticularis.
Complimentary Contributor Copy