
Page 398 - The Vasculitides, Volume 1: General Considerations and Systemic Vasculitis
P. 398
372 Rami N. Al-Rohil and J. Andew Carlson
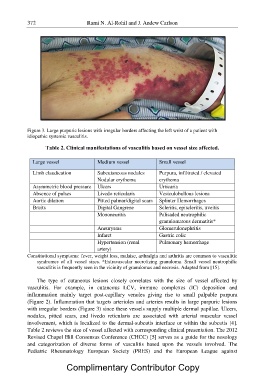
Figure 3. Large purpuric lesions with irregular borders affecting the left wrist of a patient with
idiopathic systemic vasculitis.
Table 2. Clinical manifestations of vasculitis based on vessel size affected.
Large vessel Medium vessel Small vessel
Limb claudication Subcutaneous nodules Purpura, infiltrated / elevated
Nodular erythema erythema
Asymmetric blood pressure Ulcers Urticaria
Absence of pulses Livedo reticularis Vesiculobullous lesions
Aortic dilation Pitted palmar/digital scars Splinter Hemorrhages
Bruits Digital Gangrene Scleritis, episcleritis, uveitis
Mononeuritis Palisaded neutrophilic
granulomatous dermatitis*
Aneurysms Glomerulonephritis
Infarct Gastric colic
Hypertension (renal Pulmonary hemorrhage
artery)
Constitutional symptoms: fever, weight loss, malaise, arthralgia and arthritis are common to vasculitic
syndromes of all vessel sizes. *Extravascular necrotizing granuloma. Small vessel neutrophilic
vasculitis is frequently seen in the vicinity of granulomas and necrosis. Adapted from [15].
The type of cutaneous lesions closely correlates with the size of vessel affected by
vasculitis. For example, in cutaneous LCV, immune complexes (IC) deposition and
inflammation mainly target post-capillary venules giving rise to small palpable purpura
(Figure 2). Inflammation that targets arterioles and arteries results in large purpuric lesions
with irregular borders (Figure 3) since these vessels supply multiple dermal papillae. Ulcers,
nodules, pitted scars, and livedo reticularis are associated with arterial muscular vessel
involvement, which is localized to the dermal-subcutis interface or within the subcutis [4].
Table 2 reviews the size of vessel affected with corresponding clinical presentation. The 2012
Revised Chapel Hill Consensus Conference (CHCC) [5] serves as a guide for the nosology
and categorization of diverse forms of vasculitis based upon the vessels involved. The
Pediatric Rheumatology European Society (PRES) and the European League against
Complimentary Contributor Copy