
Page 343 - The Vasculitides, Volume 1: General Considerations and Systemic Vasculitis
P. 343
Giant Cell Arteritis 317
studies note aortic aneurysm and dissection in 3% to 18% of patients with GCA [66-70]. In a
cross-sectional study employing CT, 12/54 (22.2%) patients with GCA developed aortic
aneurysms after 4 to 10.5 years [63] with relative risks (RR) ranging from 3 to 17.3 [66, 71].
Distal stenotic lesions of the subclavian, axillary and brachial arteries occur in 3% to 15% of
patients [51, 67, 72, 73]. Lower extremity arteries are infrequently affected [67], however the
identification of claudication and vascular bruits is important to ascertain before initiation of
empiric glucocorticoids because such findings, which add weight to the formal diagnosis of
GCA, may resolve with effective treatment [70, 74]. The management of peripheral arterial
involvement rarely requires surgical intervention [55, 70, 75].
Diagnosis
Classification Criteria
The American College of Rheumatology (ACR) 1990 criteria for the classification of
GCA [76] required the presence of three or more of the following including, age >50 years,
new onset localized headache, temporal artery tenderness or decreased pulsation, erythrocyte
sedimentation rate (ESR) >50 mm/hr, and abnormal TAB, yielding a sensitivity of 93.5% and
specificity of 91.2% to discern GCA from other vasculitides.
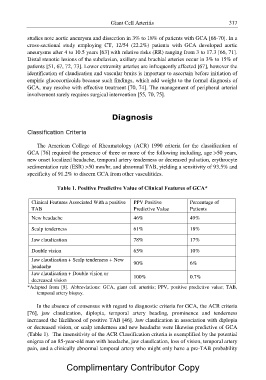
Table 1. Positive Predictive Value of Clinical Features of GCA*
Clinical Features Associated With a positive PPV Positive Percentage of
TAB Predictive Value Patients
New headache 46% 49%
Scalp tenderness 61% 18%
Jaw claudication 78% 17%
Double vision 65% 10%
Jaw claudication + Scalp tenderness + New 90% 6%
headache
Jaw claudication + Double vision or 100% 0.7%
decreased vision
*Adapted from [8]. Abbreviations: GCA, giant cell arteritis; PPV, positive predictive value; TAB,
temporal artery biopsy.
In the absence of consensus with regard to diagnostic criteria for GCA, the ACR criteria
[76], jaw claudication, diplopia, temporal artery beading, prominence and tenderness
increased the likelihood of positive TAB [46]. Jaw claudication in association with diplopia
or decreased vision, or scalp tenderness and new headache were likewise predictive of GCA
(Table 1). The insensitivity of the ACR Classification criteria is exemplified by the potential
enigma of an 85-year-old man with headache, jaw claudication, loss of vision, temporal artery
pain, and a clinically abnormal temporal artery who might only have a pre-TAB probability
Complimentary Contributor Copy