
Page 259 - The Vasculitides, Volume 1: General Considerations and Systemic Vasculitis
P. 259
Cryoglobulinemic Vasculitis 233
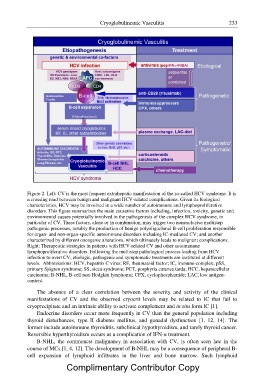
Figure 2. Left: CV is the most frequent extrahepatic manifestation of the so-called HCV syndrome. It is
a crossing road between benign and malignant HCV-related complications. Given its biological
characteristics, HCV may be involved in a wide number of autoimmune and lymphoproliferative
disorders. This figure summarizes the main causative factors including, infection, toxicity, genetic and
environmental causes potentially involved in the pathogenesis of the complex HCV syndrome, in
particular of CV. These factors, alone or in combination, may trigger two nonexclusive multistep
pathogenic processes, notably the production of benign polyoligoclonal B-cell proliferation responsible
for organ- and non-organ-specific autoimmune disorders including IC-mediated CV; and another
characterized by different oncogenic alterations, which ultimately leads to malignant complications.
Right: Therapeutic strategies in patients with HCV-related CV and other autoimmune
lymphoproliferative disorders. Following the multistep pathological process leading from HCV
infection to overt CV, etiologic, pathogenic and symptomatic treatments are instituted at different
levels. Abbreviations: HCV, hepatitis C virus; RF, rheumatoid factor; IC, immune-complex; pSS,
primary Sjögren syndrome; SS, sicca syndrome; PCT, porphyria cutanea tarda; HCC, hepatocellular
carcinoma; B-NHL, B-cell non-Hodgkin lymphoma; CPX, cyclophosphamide; LAC, low antigen-
content.
The absence of a clear correlation between the severity and activity of the clinical
manifestations of CV and the observed cryocrit levels may be related to IC that fail to
cryoprecipitate and an intrinsic ability to activate complement and in situ form IC [1].
Endocrine disorders occur more frequently in CV than the general population including
thyroid disturbances, type II diabetes mellitus, and gonadal dysfunction [1, 12, 14]. The
former include autoimmune thyroiditis, subclinical hypothyroidism, and rarely thyroid cancer.
Reversible hyperthyroidism occurs as a complication of IFN-? treatment.
B-NHL, the commonest malignancy in association with CV, is often seen late in the
course of MCs [1, 4, 12]. The development of B-NHL may be a consequence of peripheral B-
cell expansion of lymphoid infiltrates in the liver and bone marrow. Such lymphoid
Complimentary Contributor Copy