
Page 256 - The Vasculitides, Volume 1: General Considerations and Systemic Vasculitis
P. 256
230 Clodoveo Ferri, Dilia Giuggioli and Marco Sebastiani
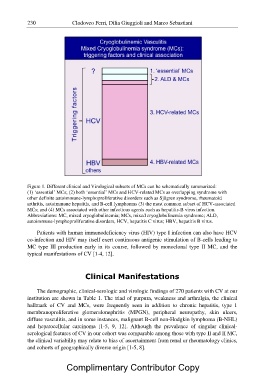
Figure 1. Different clinical and Virological subsets of MCs can be schematically summarized:
(1) „essential? MCs; (2) both „essential? MCs and HCV-related MCs as overlapping syndrome with
other definite autoimmune-lymphoproliferative disorders such as Sjögren syndrome, rheumatoid
arthritis, autoimmune hepatitis, and B-cell lymphomas (3) the most common subset of HCV-associated
MCs; and (4) MCs associated with other infectious agents such as hepatitis-B virus infection.
Abbreviations: MC, mixed cryoglobulinemia; MCs, mixed cryoglobulinemia syndrome; ALD,
autoimmune-lymphoproliferative disorders, HCV, hepatitis C virus; HBV, hepatitis B virus.
Patients with human immunodeficiency virus (HIV) type I infection can also have HCV
co-infection and HIV may itself exert continuous antigenic stimulation of B-cells leading to
MC type III production early in its course, followed by monoclonal type II MC, and the
typical manifestations of CV [1-4, 12].
Clinical Manifestations
The demographic, clinical-serologic and virologic findings of 270 patients with CV at our
institution are shown in Table 1. The triad of purpura, weakness and arthralgia, the clinical
hallmark of CV and MCs, were frequently seen in addition to chronic hepatitis, type 1
membranoproliferative glomerulonephritis (MPGN), peripheral neuropathy, skin ulcers,
diffuse vasculitis, and in some instances, malignant B-cell non-Hodgkin lymphoma (B-NHL)
and hepatocellular carcinoma [1-5, 9, 12]. Although the prevalence of singular clinical-
serological features of CV in our cohort was comparable among those with type II and II MC,
the clinical variability may relate to bias of ascertainment from renal or rheumatology clinics,
and cohorts of geographically diverse origin [1-5, 8].
Complimentary Contributor Copy